6 Recurrent Events & Multi-State Models
When subjects experience the same event more than once (recurrent hospitalisations, infections, relapses), standard Cox regression is invalid because it assumes one event per subject. This module provides three recurrent-event frameworks and a multi-state modelling approach.
6.1 Recurrent Event Models
| Model | Assumption | Strengths | Limitations |
|---|---|---|---|
| Andersen-Gill (AG) | Events are independent | Simple extension of Cox | Ignores event ordering |
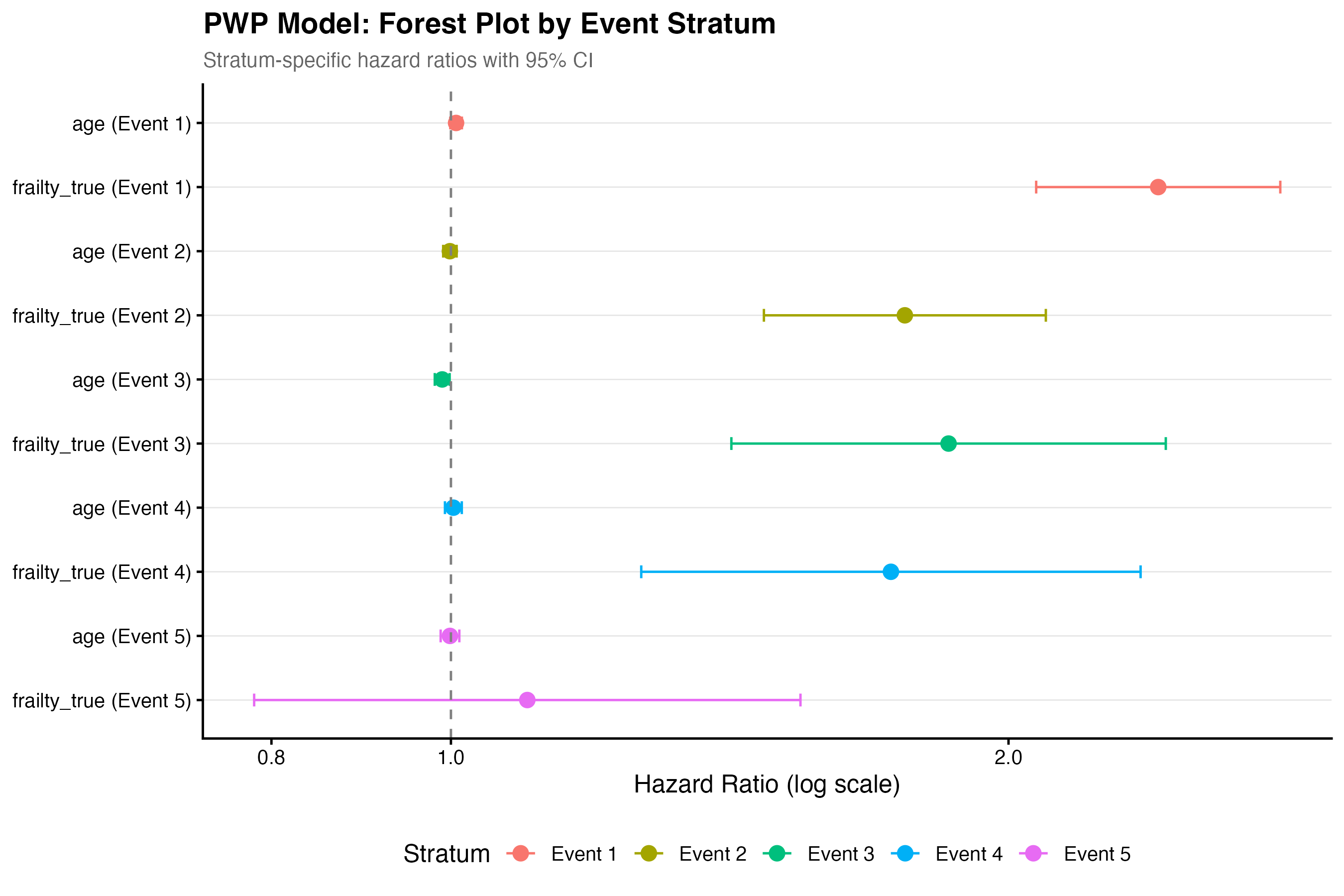
| Prentice-Williams-Peterson (PWP) | Event-order matters | Stratifies by event number | Sparse data in later strata |
| Wei-Lin-Weissfeld (WLW) | Marginal model | Robust to dependence structure | Less efficient |
| Frailty | Subject-level random effect | Models heterogeneity | Distributional assumption |
AG is the default for recurrent events. Use PWP when event ordering is clinically meaningful (e.g., 1st vs 2nd relapse differs). Use frailty when between-subject heterogeneity is the scientific question1.
6.2 Script Pipeline
| Script | Purpose |
|---|---|
01_recurrent_descriptive.R |
Event frequency tables, gap-time summaries |
02_ag_model.R |
Andersen-Gill counting process model |
03_pwp_model.R |
Prentice-Williams-Peterson gap-time model |
04_wlw_model.R |
Wei-Lin-Weissfeld marginal model |
05_frailty_recurrent.R |
Gamma frailty for recurrent events |
06_multistate_setup.R |
Define states and transitions with mstate |
07_multistate_models.R |
Fit transition-specific Cox models |
08_multistate_plots.R |
State occupation probabilities |
6.3 Andersen-Gill Example
library(survival)
ag_fit <- coxph(
Surv(tstart, tstop, status) ~ group + age + cluster(id),
data = df_counting
)
summary(ag_fit)The cluster(id) term provides robust sandwich standard errors to account for within-subject correlation.
6.4 Multi-State Models
For complex disease trajectories (e.g., healthy -> diseased -> dead, with possible recovery), the multi-state module uses the mstate package:
library(mstate)
tmat <- transMat(x = list(c(2, 3), c(3), c()),
names = c("Healthy", "Disease", "Dead"))
msdata <- msprep(data = df, trans = tmat,
time = c(NA, "t_disease", "t_death"),
status = c(NA, "s_disease", "s_death"))Script 08_multistate_plots.R generates stacked state-occupation probability plots — useful for showing how the proportion of patients in each state evolves over time.
6.5 Running the Module
make analyze-recurrent PROJECT=my-study6.6 Demo: Recurrent Events (Scenario 3)
N=400 patients with up to 5 recurrent infections and terminal death event. Gamma frailty (variance=0.5).
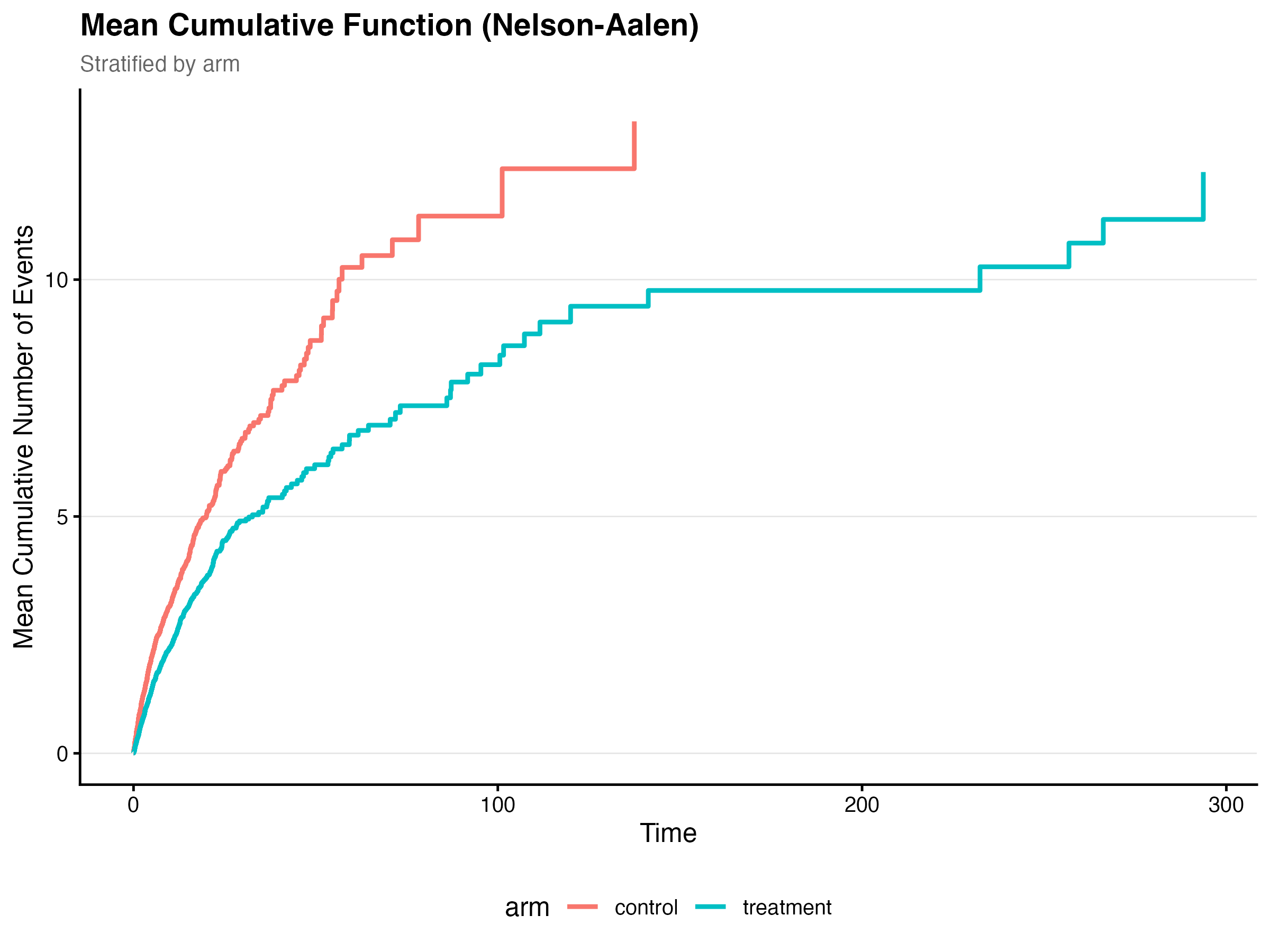
6.6.1 Mean Cumulative Function
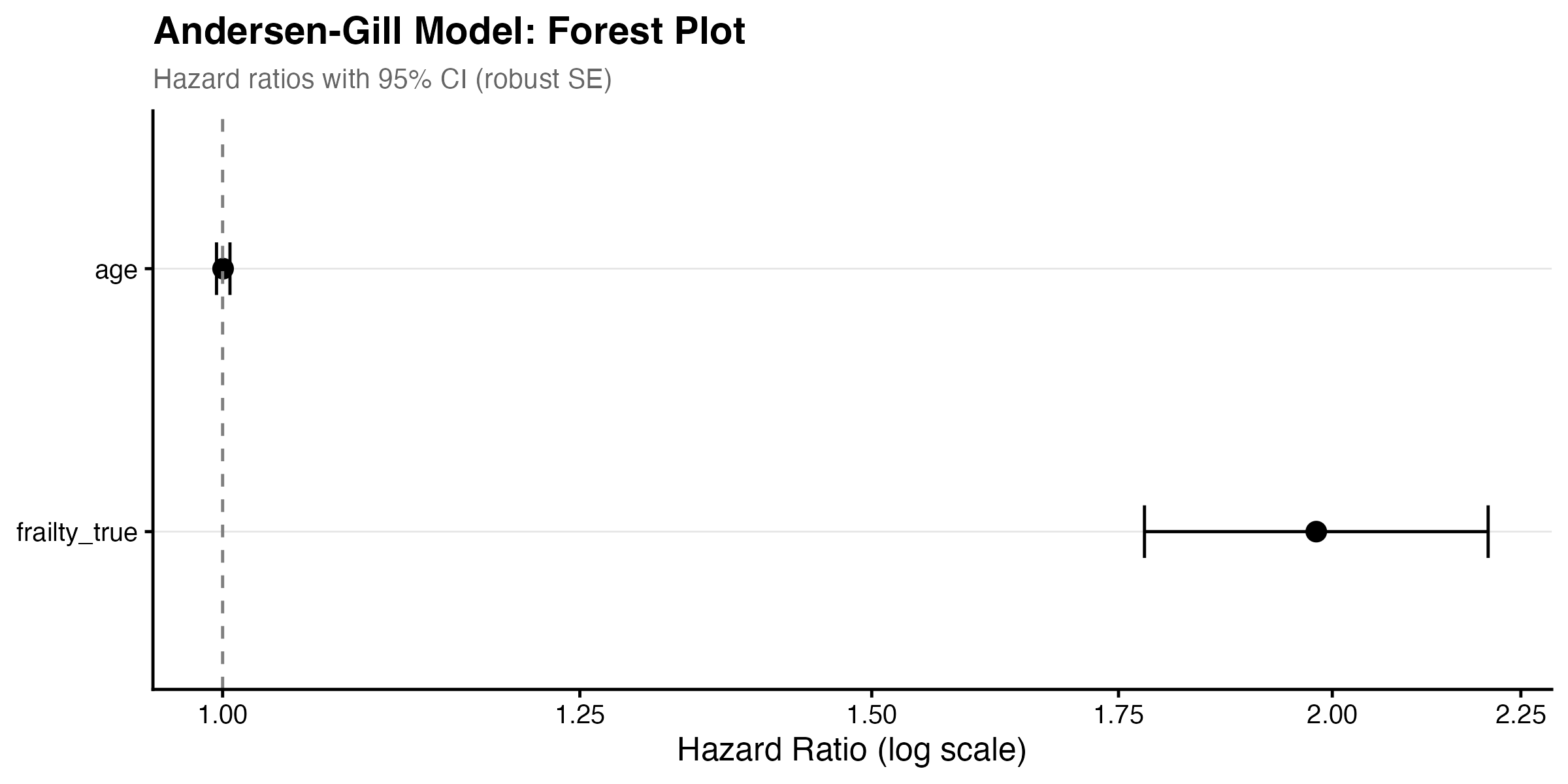
6.6.2 Model Comparison
The Andersen-Gill model estimated a frailty HR of 1.98 (95% CI: 1.78–2.20, p < 0.001), confirming that higher underlying frailty strongly predicts recurrent infections. Age was non-significant (HR = 1.00, p = 0.87). Event rates differed substantially between arms: control 0.254 events/person-time (651 events across 204 subjects) versus treatment 0.148 events/person-time (551 events across 196 subjects).
| Variable | HR | 95% CI | p-value |
|---|---|---|---|
| Frailty (true) | 1.98 | 1.78–2.20 | < 0.001 |
| Age | 1.00 | 1.00–1.00 | 0.870 |
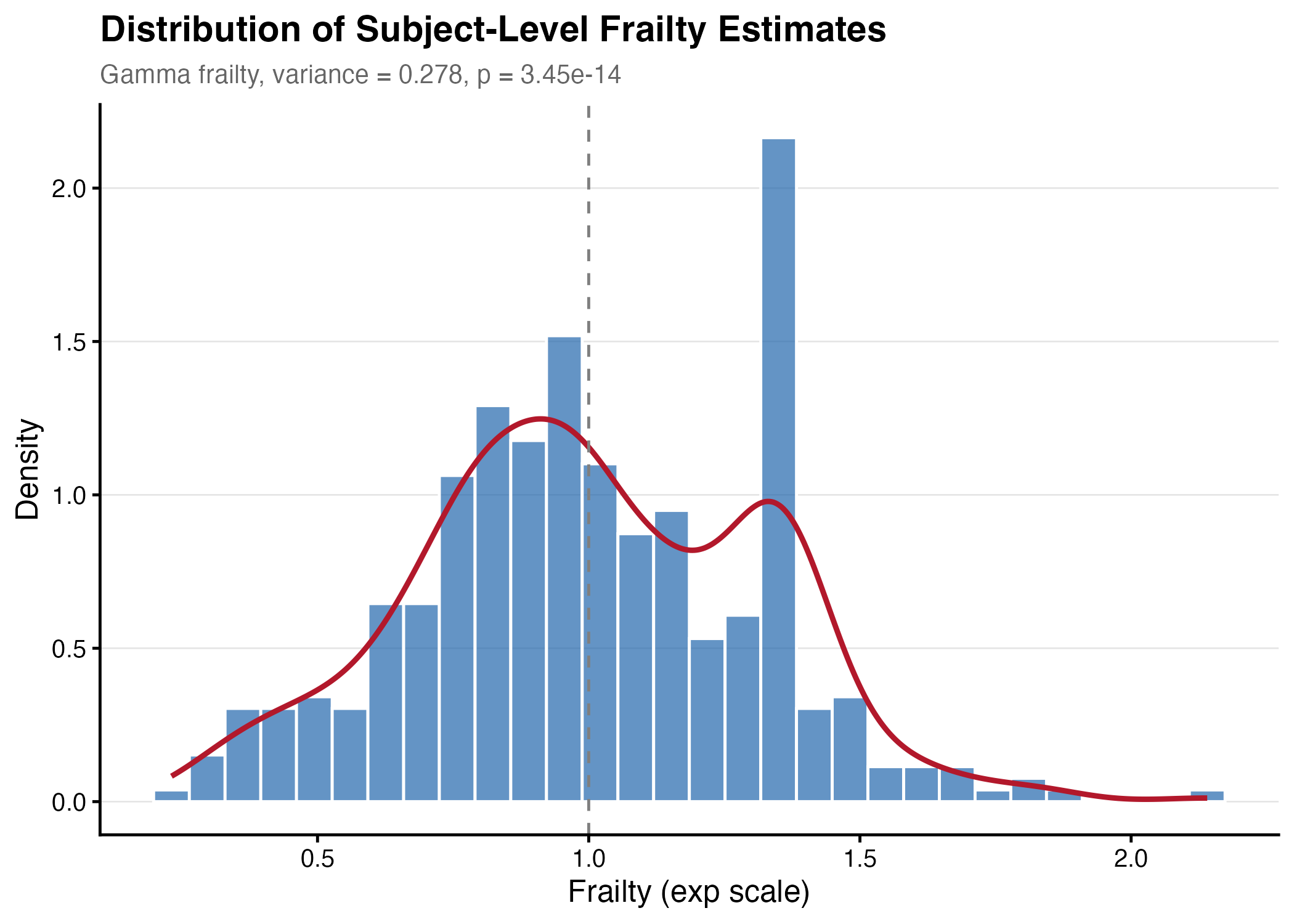
6.6.3 Frailty Estimation
The gamma frailty model estimated a frailty variance of 0.278, which is lower than the true simulated variance of 0.50. This attenuation is expected — frailty variance is notoriously difficult to estimate and tends to be biased downward in finite samples.
6.6.4 Terminal Event