Does TLS at presentation predict worse outcome in lymphoma?
A rapid evidence synthesis · 6 cohorts · 857 patients
April 11, 2026
From search to synthesis — 766 → 6
Five filtering steps
- Merge two databases
- DOI + fuzzy title dedupe
- Title pre-filter ⚠️
- AI abstract screen
- Full-text eligibility
Step 3 is the non-standard one — 611 records excluded on title alone. Recall gap, documented in limitations.

Headline result — Pool F minus Alavi (k = 5)
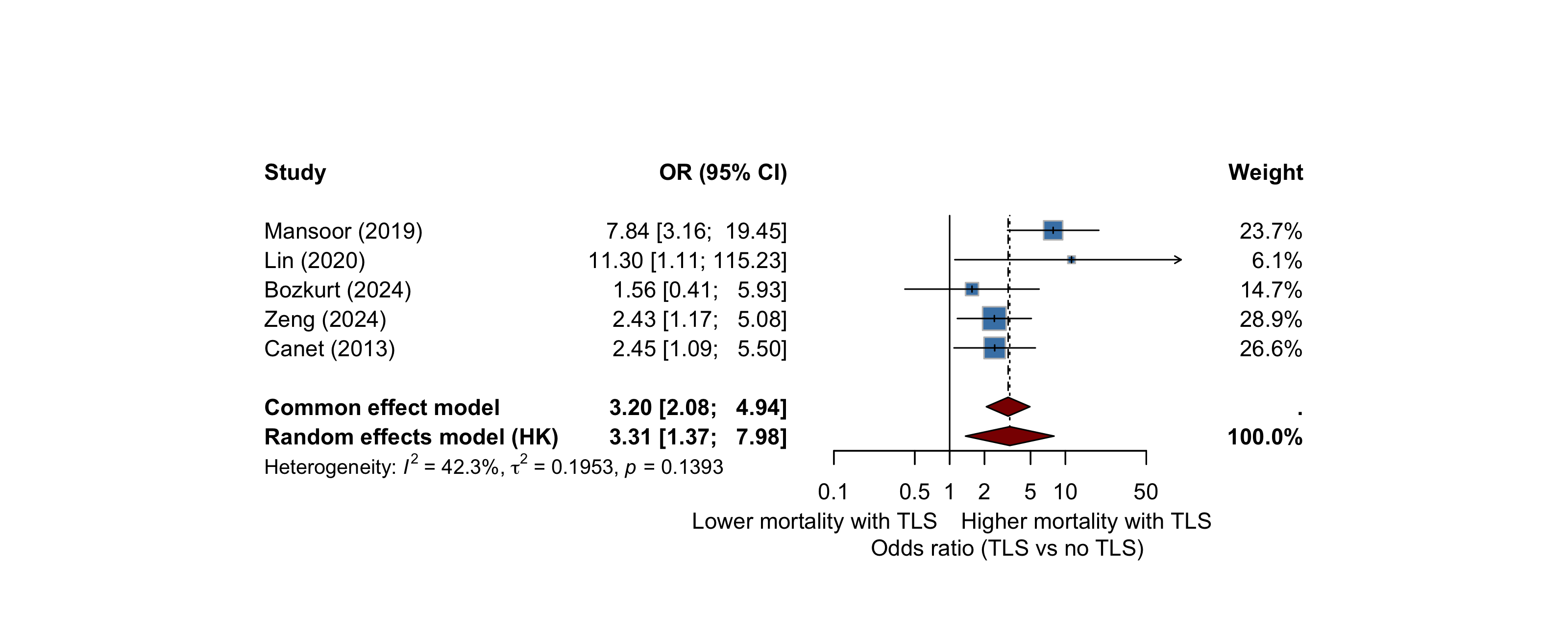
OR 3.31 (95 % CI 1.37 – 7.98), p = 0.020, I² = 42 %
Across the five studies we are willing to defend on their own merits, TLS at presentation triples the odds of mortality in lymphoma patients.
Why one number isn’t enough
Stratify by adjustment × time window
Every leaf is k ≤ 2.
The OR 3.3 only exists when we average methodologically heterogeneous studies together.
→ no sub-pool is statistically robust on its own

Bedside decision pathway
Two questions decide everything
- When did TLS appear?
- Is there organ dysfunction?
Everything downstream — ward vs ICU, timing of rasburicase, chemotherapy delay — follows from these two answers.
