ASH 2025 B-Cell Lymphoma Updates
MCL, MZL, and Waldenström Macroglobulinemia
2025-12-01
First‐line treatment of mantle cell lymphoma.
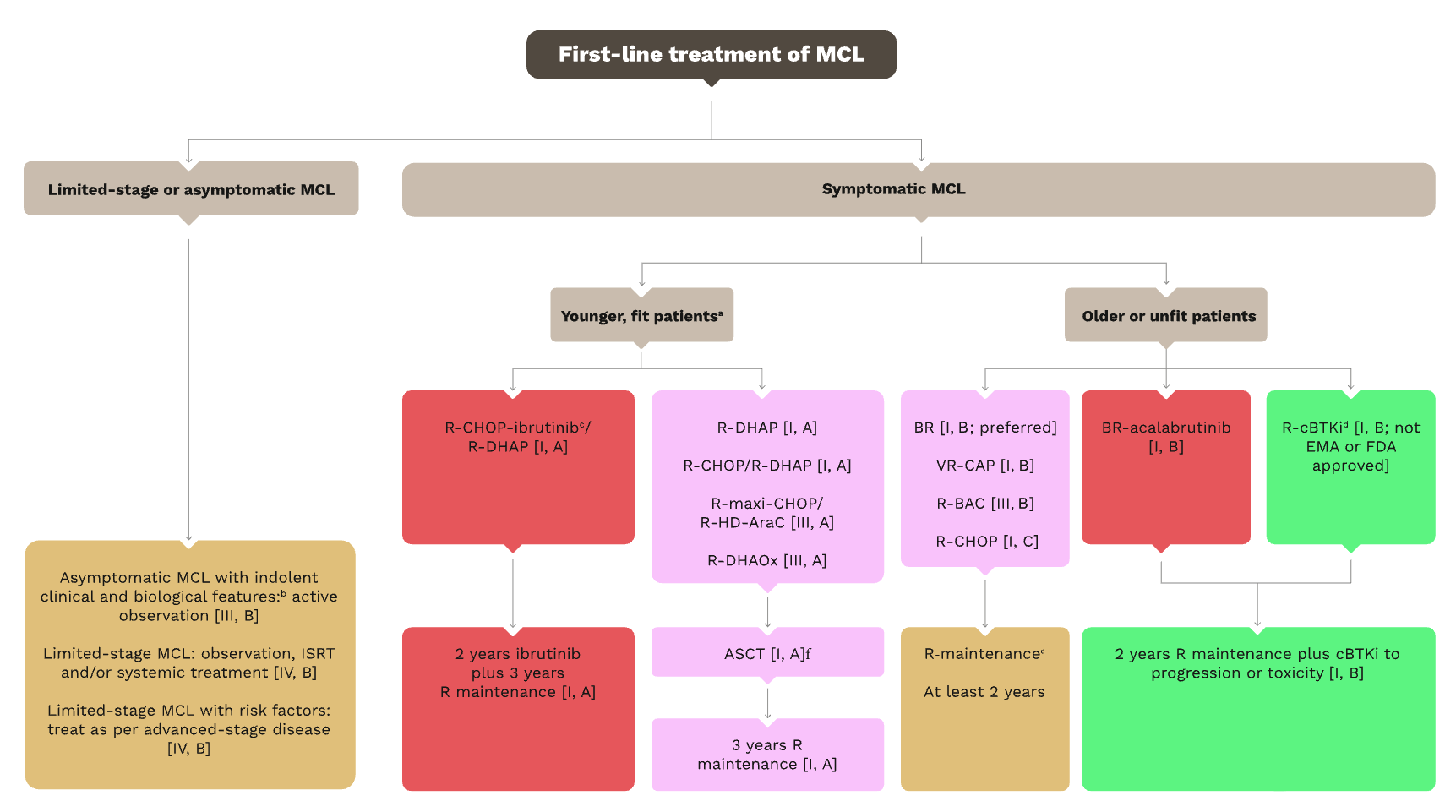
Caption: First‐line treatment of mantle cell lymphoma.
ECHO trial: Acalabrutinib + BR for frontline MCL
Phase III (NCT02972840)
Background
- Transplant-ineligible untreated MCL 1
- N=598 patients, median follow-up 50 months
Method
- Acalabrutinib 100mg BID + Bendamustine-Rituximab
- versus Placebo + BR
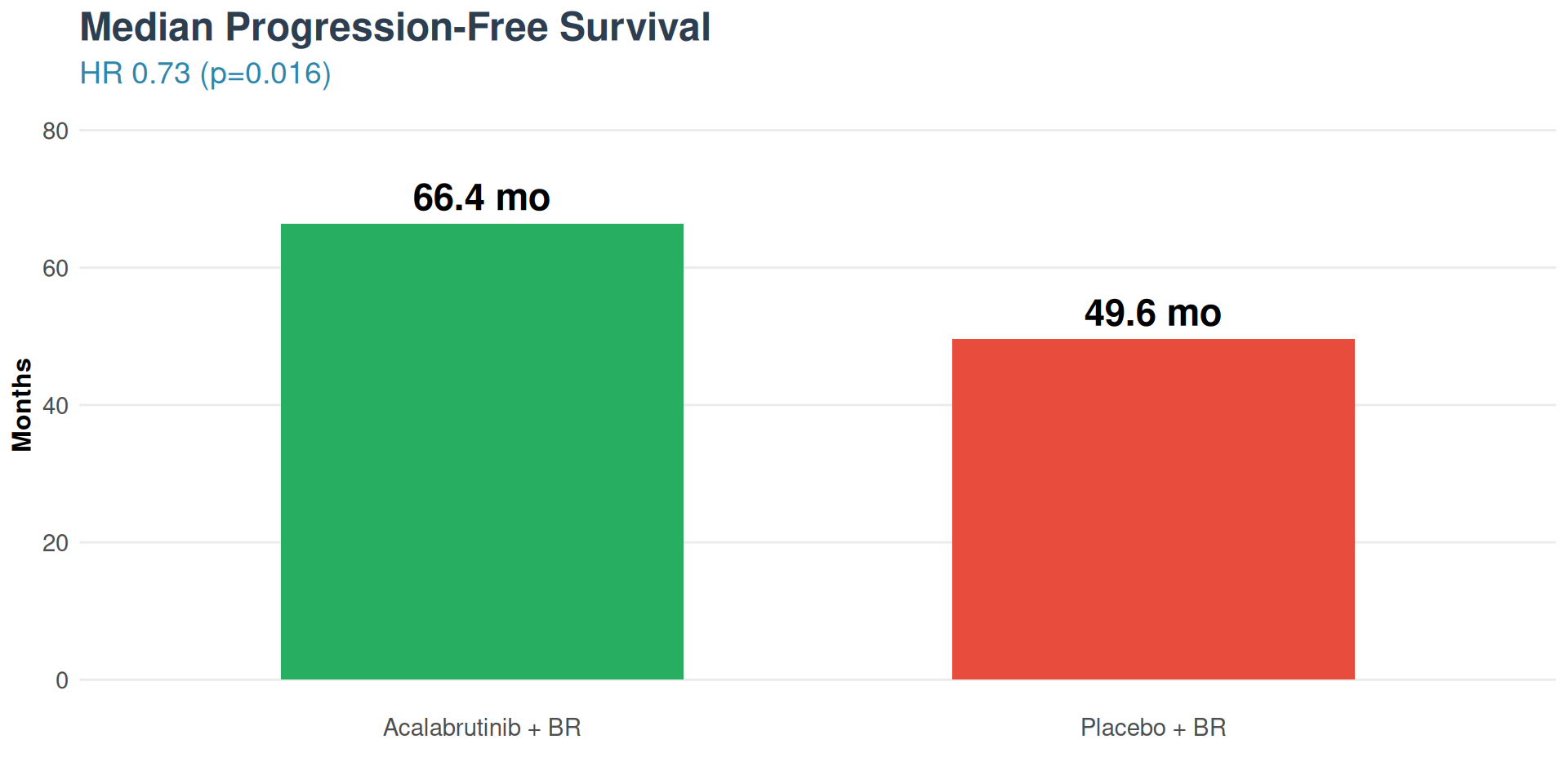
Results
- mPFS: 66.4 versus 49.6 months
- HR 0.73 (95% CI 0.57-0.94, p=0.016)
- 27% reduction in progression/death risk
- Ki-67 ≥30%: HR 0.69 (high proliferation benefit)
ECHO Trial: Safety & Regulatory
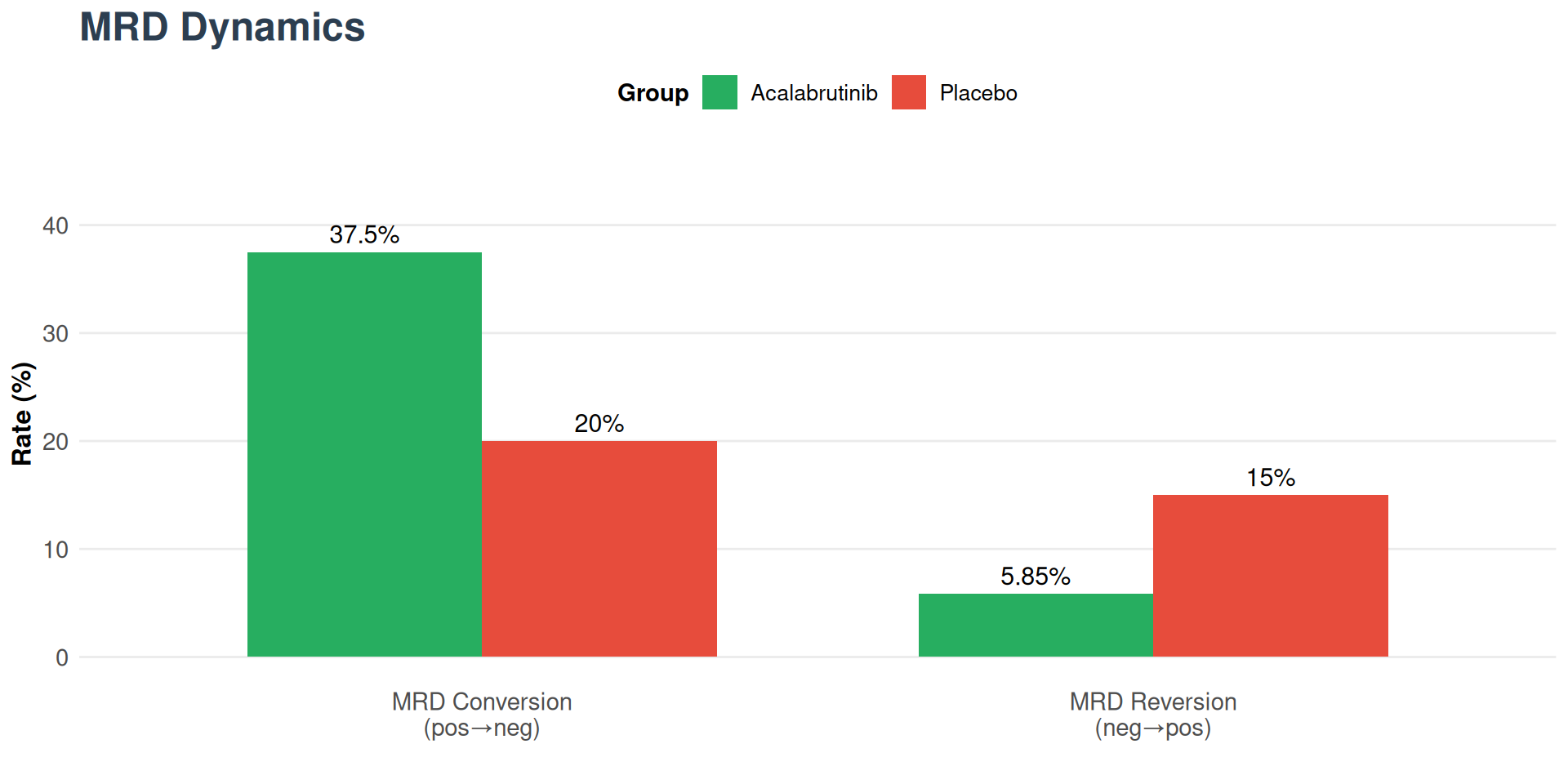
Additional Efficacy Data
Regulatory Status
- FDA Traditional Approval: January 16, 2025
- Approved for transplant-ineligible untreated MCL
- Converted from accelerated approval
- EMA Approval: May 6, 2025
- Project Orbis international review collaboration
Subgroup Analysis
- TP53 mutant: HR 0.88 (modest benefit)
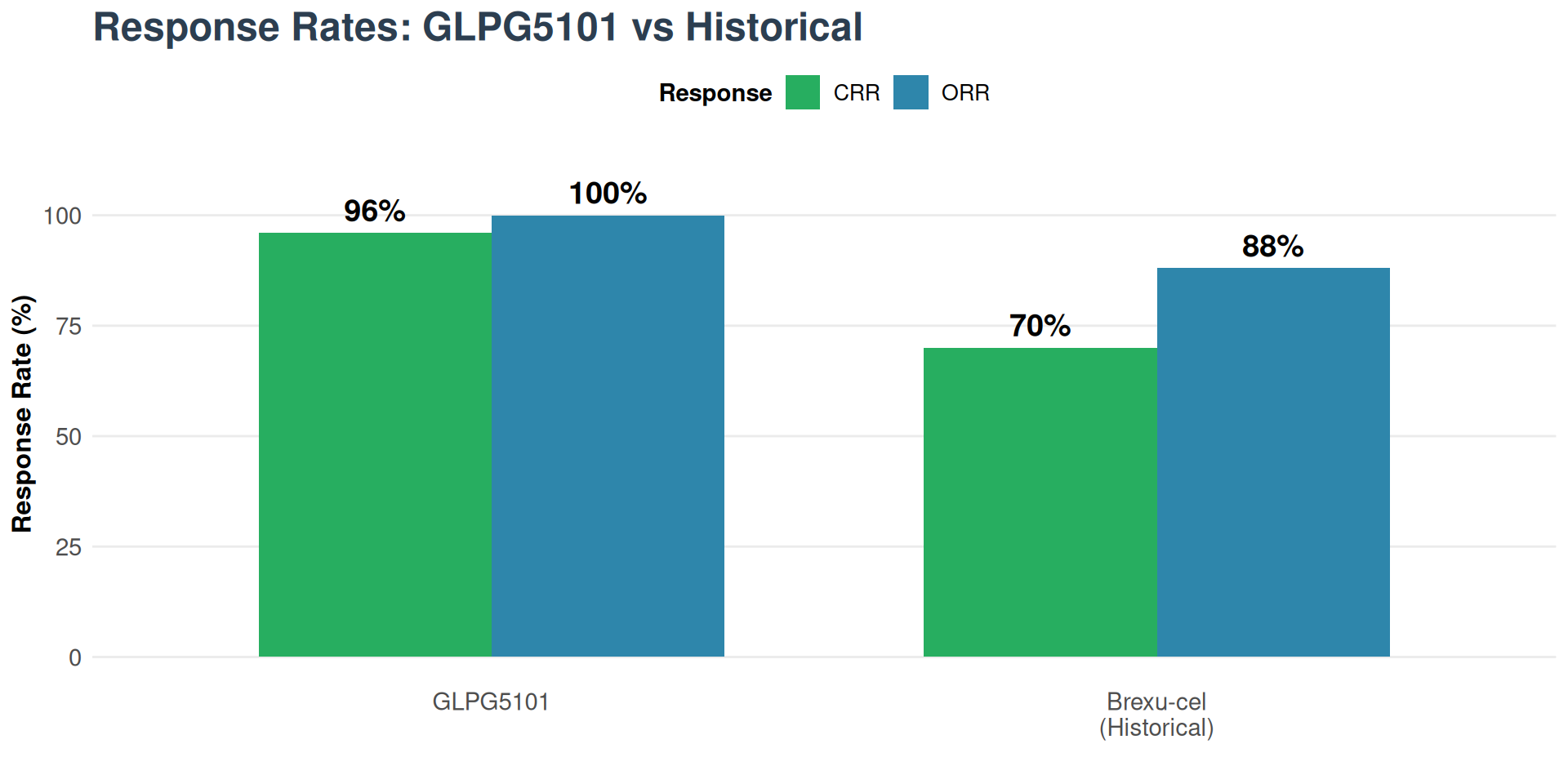
- ORR: 91% vs 88%
- CR rate: 66.6% vs 53.5%
PFS and OS with and without COVID-19 deaths and PFS by acalabrutinib exposure
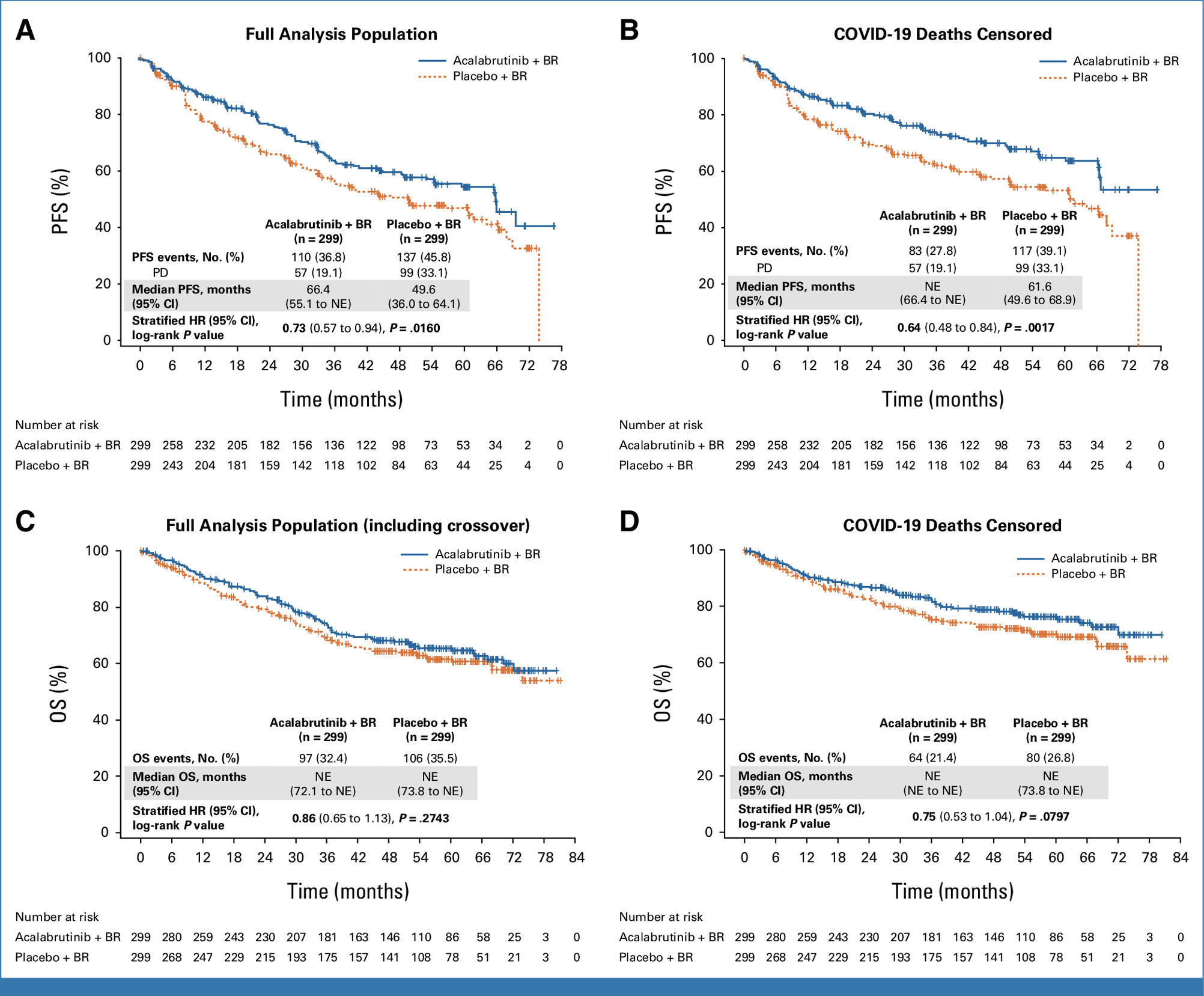
Wang M, Salek D, Belada D, et al. Acalabrutinib Plus Bendamustine-Rituximab in Untreated Mantle Cell Lymphoma. Journal of Clinical Oncology. 2025;43(20):2276-2284. doi:https://doi.org/10.1200/jco-25-00690
BOVen: Safety & Guideline Update
Safety Profile
| Adverse Event | Rate |
|---|---|
| Diarrhea | 64% (mostly low-grade) |
| COVID-19 infection | 56% |
| Infusion reaction | 24% |
| Neutropenia | 32% |
| Grade 4 TRAEs | 0% |
- Time-limited therapy possible with MRD guidance
- No treatment discontinuation due to toxicity
Regulatory & Guidelines
NCCN Category 2A
BOVen now included for TP53-mutant MCL
- Published in Blood January 2025
- Expansion cohort: additional 25 patients enrolling
- Paradigm shift for high-risk MCL
- First effective chemo-free option for TP53-MCL
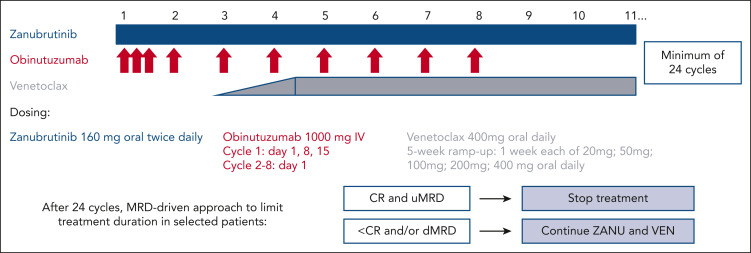
MAVO: Acalabrutinib + Venetoclax + Obinutuzumab
Phase I/II (NCT04855695)
Populations
- R/R MCL (n=18)
- Treatment-naïve (n=21)
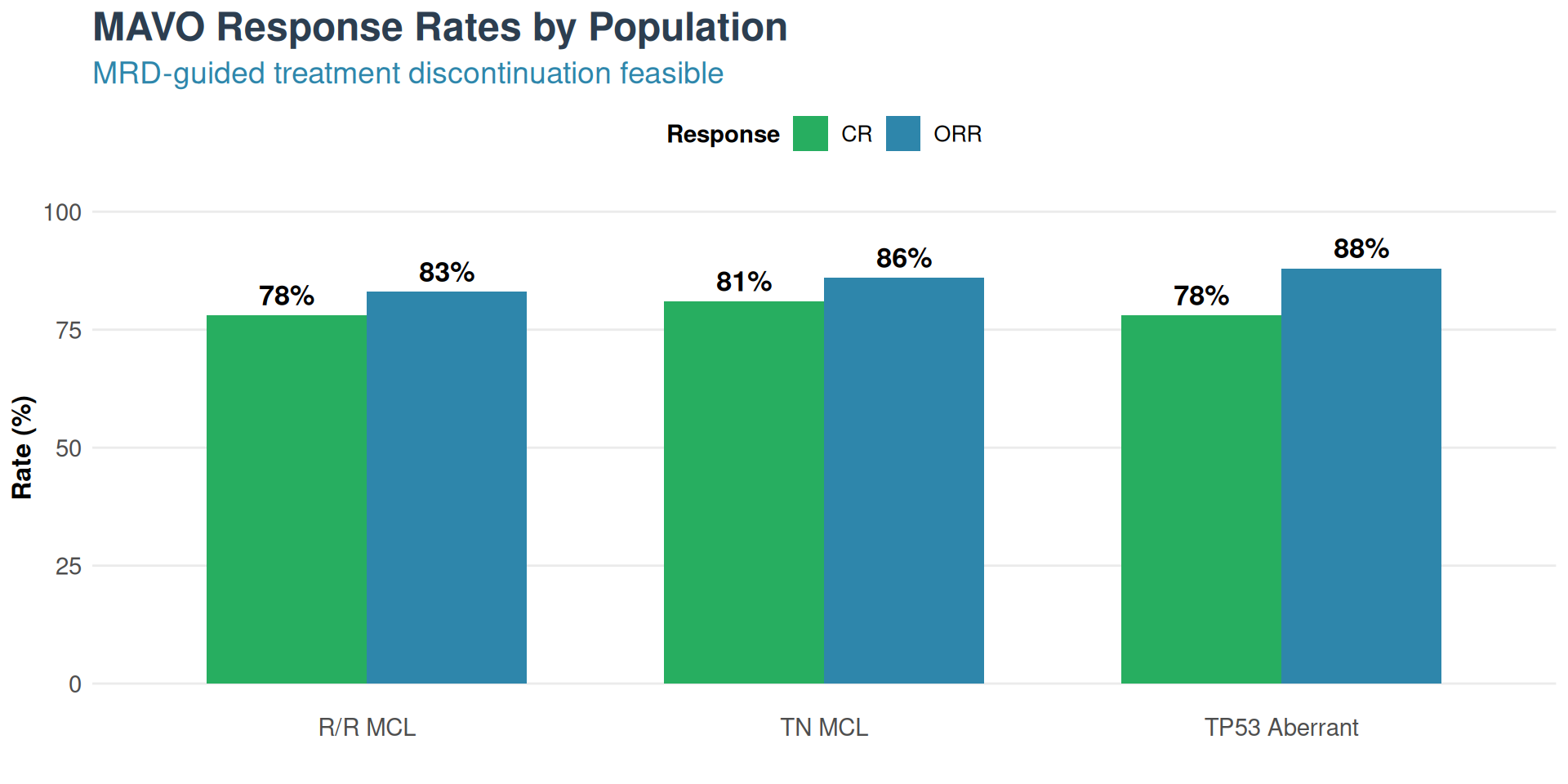
Results - R/R MCL
- ORR: 83%, CR: 78%
- 18-month PFS: 77%
Results - Treatment-Naïve
- ORR: 86%, CR: 81%
- TP53 aberrant (n=8): 88% ORR
- MRD-negative CR: 86%
- TP53 MRD-neg CR: 91%
Pirtobrutinib: Safety & Regulatory
Safety Profile
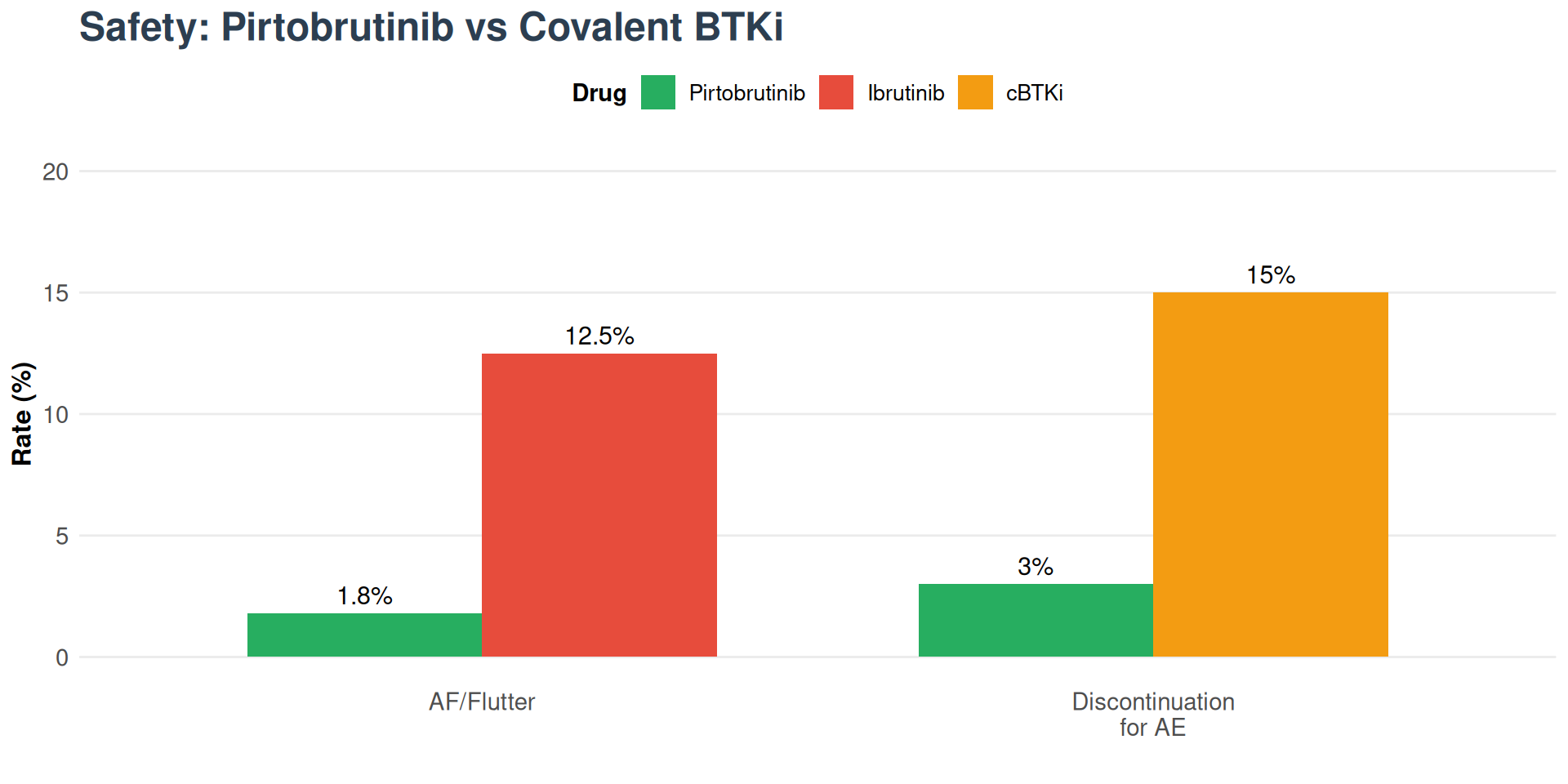
Regulatory Status
FDA Full Approval
December 3, 2025 - Converted from accelerated approval (Dec 2023)
- First-in-class non-covalent BTKi
- Phase III BRUIN MCL-321 ongoing (vs cBTKi in BTKi-naïve R/R MCL)
Waldenström Activity
- MRR: 71.3% in prior cBTKi patients
- MRR: 66.7% in cBTKi-refractory
- Off-label NCCN support for prior-treated WM
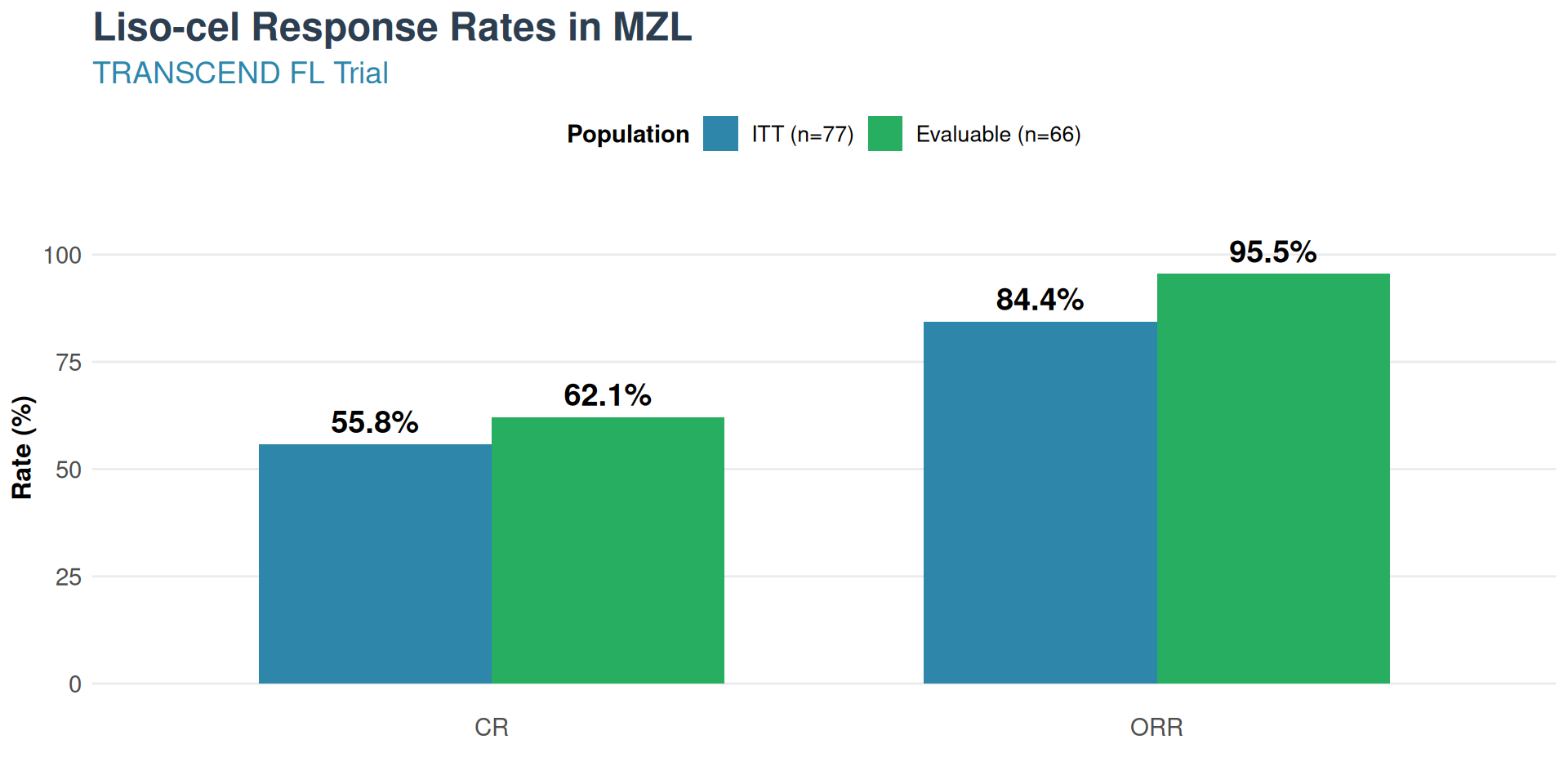
Liso-cel: First CAR-T approved for MZL
TRANSCEND FL (NCT04245839)
Background
- MZL ~10% of NHL, 3 subtypes 1
- No prior disease-specific approved therapy
Method
- CD19 CAR-T, 1:1 CD4:CD8 composition
- N=77 (ITT) / 66 (evaluable)
Results
- ORR: 84.4% (ITT) / 95.5% (evaluable)
- CR: 55.8% (ITT) / 62.1% (evaluable)
- 24-month DOR: 88.6% maintained
- 24-month PFS: 85.7%
- 24-month OS: 90.4%
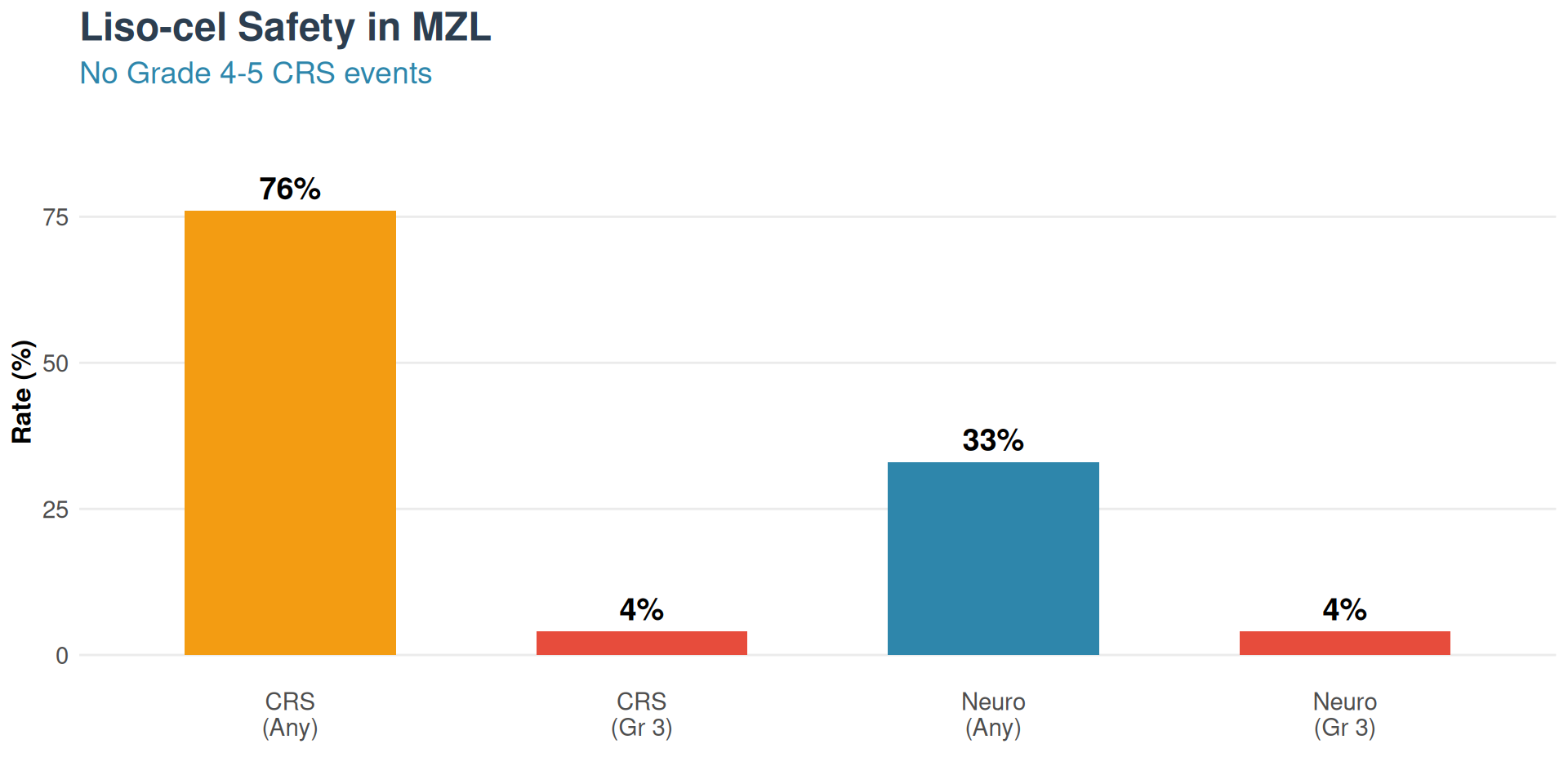
Liso-cel: Safety & FDA Approval
Safety Profile
Regulatory Status
FDA Approval: December 4, 2025
First CAR-T therapy approved for MZL
- Fifth cancer indication for Breyanzi
- Most approved indications of any CD19 CAR-T
- Requirement: ≥2 prior lines of systemic therapy
- Orphan drug designation granted
Predictable Pharmacokinetics
- Unique 1:1 CD4:CD8 defined composition
- Consistent safety across all liso-cel indications
- Lower severe neurotoxicity than other CAR-T products
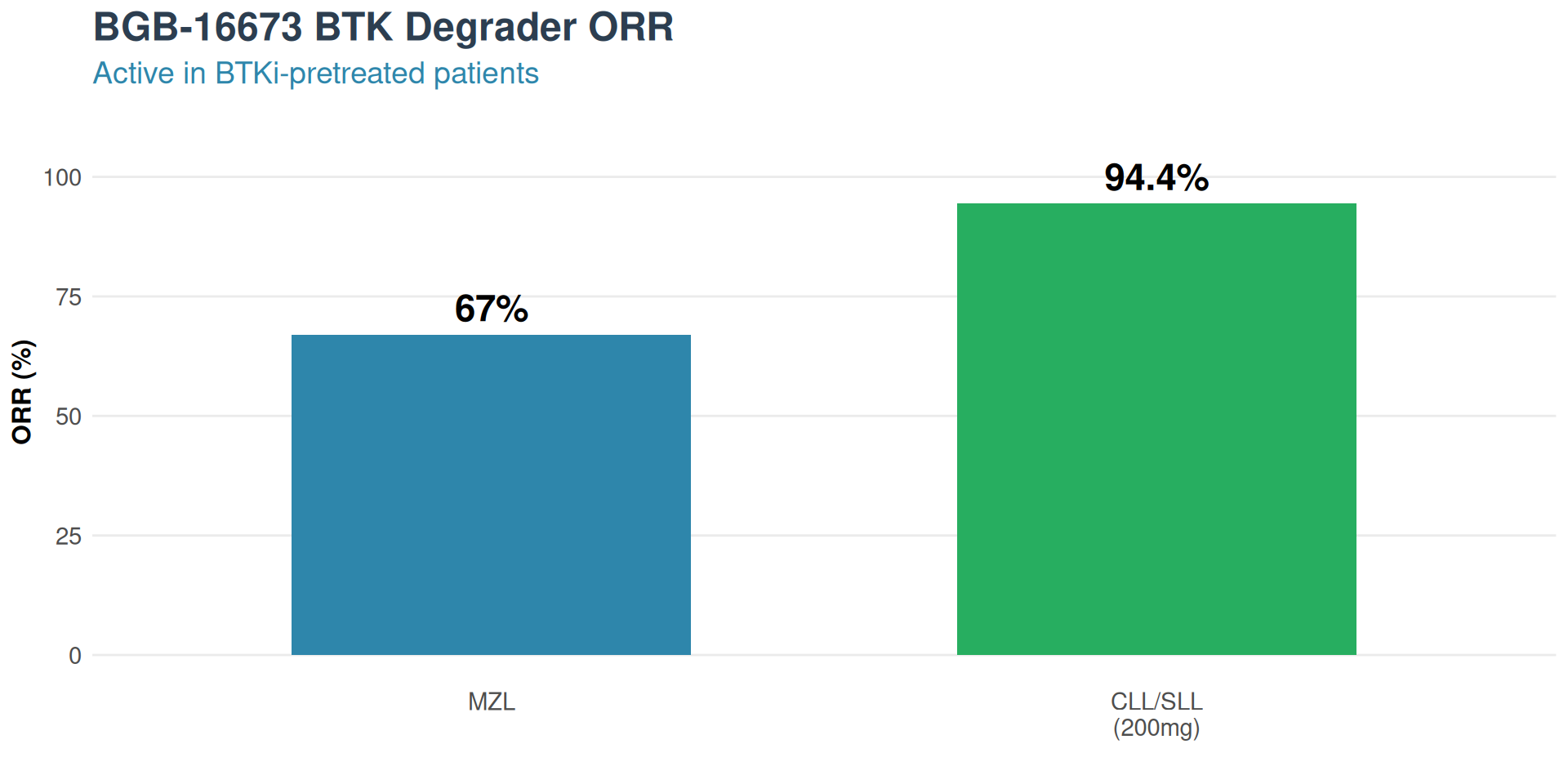
BGB-16673: BTK Degrader for BTKi-Resistant Disease
CaDAnCe-101 Trial (NCT05006716)
Mechanism
- CDAC recruits cereblon E3 ligase
- Induces BTK ubiquitination and proteasomal degradation
- Eliminates entire BTK protein (not just inhibition)
Targets
- C481S mutations
- “Kinase-dead” scaffold mutations (L528W)
- Active regardless of prior BTKi exposure
Results
- MZL ORR: 67% in response-evaluable
- CLL/SLL ORR: 94.4% at 200mg dose (RDFE)
Phase 3 trial activated: BGB-16673 vs Pirtobrutinib head-to-head
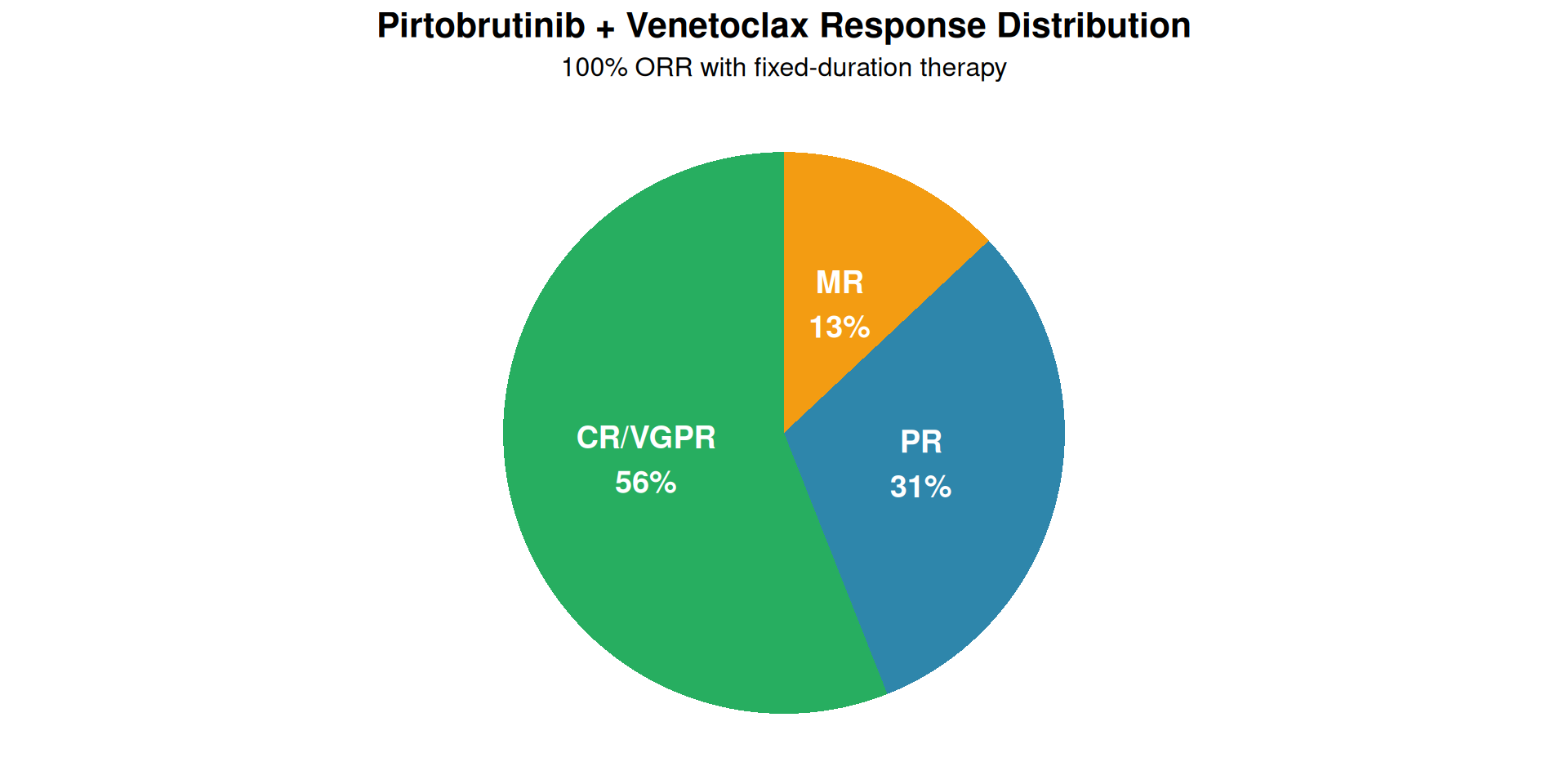
Pirtobrutinib + Venetoclax: Fixed-Duration WM Therapy
Dana-Farber Phase II
Background
- WM typically requires indefinite BTKi therapy
- Cumulative toxicities and resistance concerns
Population
- N=27 evaluable (MYD88-mutant)
- Previously treated, symptomatic
Method
- Fixed 24-cycle oral combination
Results
- ORR: 100%
- CR/VGPR: 56% (exceeds futility threshold)
- MRR: 87%
- Median time to VGPR: 1.9 months
- No arrhythmia events to date
“Depth of response beyond what was expected for each medication separately” - Dr. Jorge Castillo
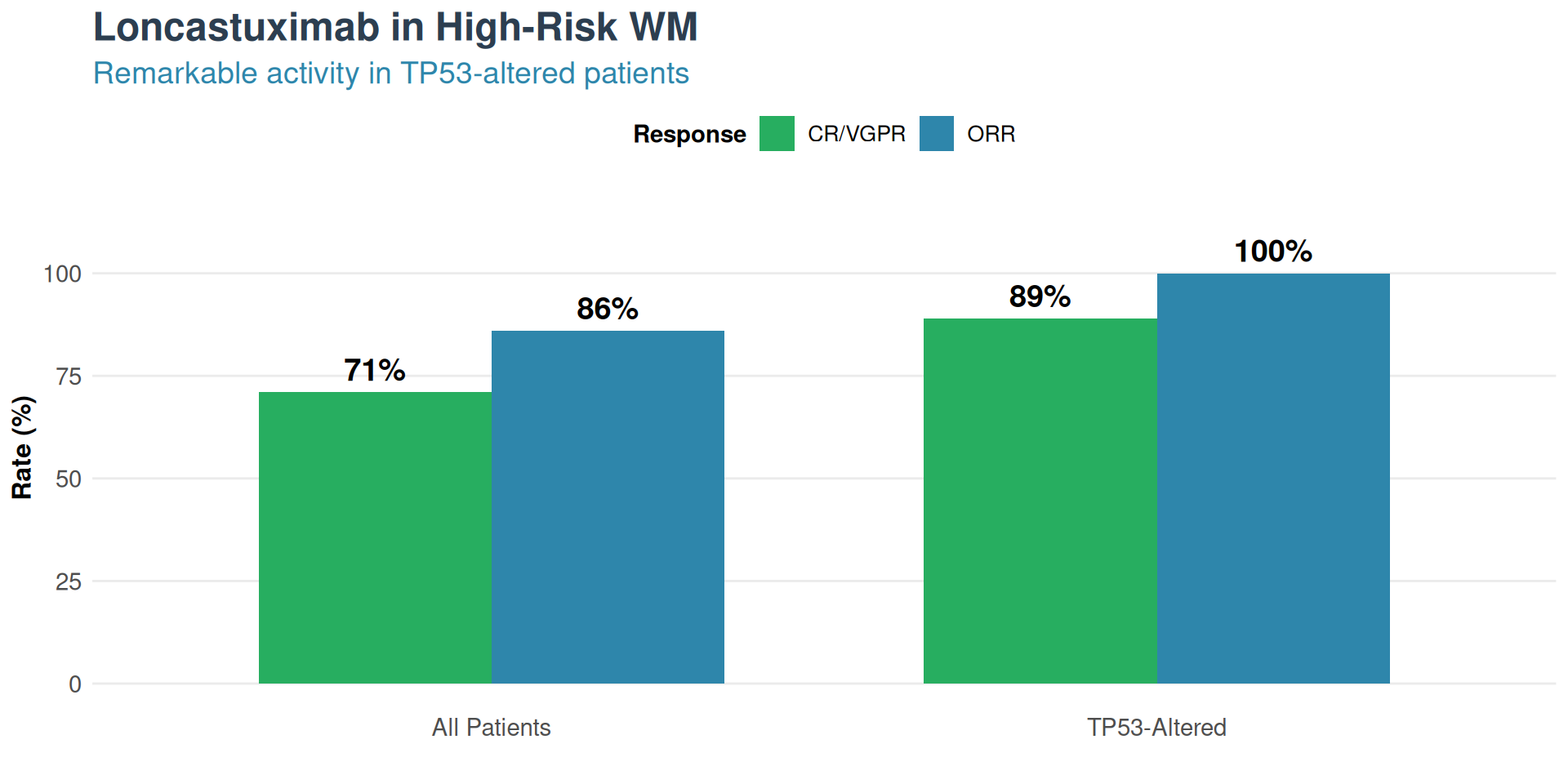
Loncastuximab Tesirine: ADC for High-Risk WM
Phase II Trial
Background
- CD19-targeting antibody-drug conjugate
- N=14, median 4 prior therapies
- High-risk: 8 CXCR4+, 8 TP53-altered
Method
- Fixed 6-dose regimen
- 150 µg/kg cycles 1-2, 75 µg/kg cycles 3-6
Results
- Overall ORR: 86%
- CR/VGPR: 71%
- TP53-altered: 100% response, 89% CR/VGPR
- Active in CXCR4-mutant (BTKi-resistant)
Note: Loncastuximab FDA-approved for DLBCL, not yet for WM